Why? Well, first of all, people die from cancer. It's the second leading cause of death in the US.
Second, it can happen to anyone. Cancer is extremely common. If they live a normal lifespan, half of women and a third of men will get it. And if you’re thinking it can’t happen to you, well—neither did the last few thousand of my patients.
Yes, we can tempt fate and increase our risk by bad lifestyle choices: alcohol, tobacco, and obesity are big risk factors. But a great many cases happen because of genetics or just bad luck. Doesn’t matter who you are, or how you vote.
Though it’s more common as we age, it can strike at any age. And it starts getting more frequent just as people enter the last decade of their working lives.
Third, it’s expensive. Though two of the most common types, breast and colon cancer, for instance, are very curable, the treatment may take 6-12 months, often interrupts work, and comes with significant out-of-pocket expenses even for those with insurance. A cancer diagnosis in the United States causes 60% of patients to have to deplete their savings, and increases the risk of bankruptcy 2 1/2 times.
So…
- Common
- Expensive
- Life & Death
That’s political dynamite.
Cancer’s been overtly political since President Nixon signed the National Cancer Act in 1971, setting in motion a half-century of public investment in cancer care.
Green Bay Oncology was founded five years after that. And we’ve seen first-hand what our citizens have gotten in return for that investment.
At a recent round table of our doctors (some retired and some still practicing), we compared life expectancies for several different cancer types from the 70s to now. Let’s consider the examples of stage 4 melanoma, kidney cancer, and colon cancer—we see they’re still uniformly fatal, but patients survive them much longer.
| DISEASE | 1970s | NOW |
| Colon Cancer | < 6 months | 2-4 years |
| Melanoma | < 6 months | 2-5 years |
| Kidney Cancer | < 6 months | 2-4 years |
| Myeloid Leukemia | 2 years | Normal lifespan |
| Promyelocytic Leukemia | < 2 weeks | Normal lifespan |
| Myeloma | 1 year | 8-10 years |
Source: Green Bay Oncology Physicians’ Roundtable, 8/2022
But several former death sentences can now be substantially delayed or cured altogether.
Next, let’s compare the patient experience of one of the most common types—breast cancer—from then until now. We can see how we’ve learned to treat it with less surgery, less side effects, and less hospitalization.
| EXPERIENCE | 1970s | NOW |
| Mastectomy | > 90% | < 30% |
| Receiving chemotherapy | > 75% | < 25% |
| Duration of chemo | 6 months | 2-3 months |
| Vomiting after chemo | > 75% | < 20% |
| Hair loss after chemo | > 50% | < 20% |
| Hospitalization after chemo | > 50% | < 10% |
Source: Green Bay Oncology Physicians’ Roundtable, 8/2022
That’s a lot of lives, workdays, and wages saved.
Almost all of this progress has been the result of publicly-funded research that started back in the 1970s. It takes a long time. We know this because besides our clinical work, Green Bay Oncology devotes significant time and resources to help test new treatments through clinical trials. Our doctors, like the people of Wisconsin, are “get involved” kind of people, and that’s why our practice is able to achieve a 17% clinical trial enrollment rate—far above the national average of 2%. This research is happening right here in our hometown.
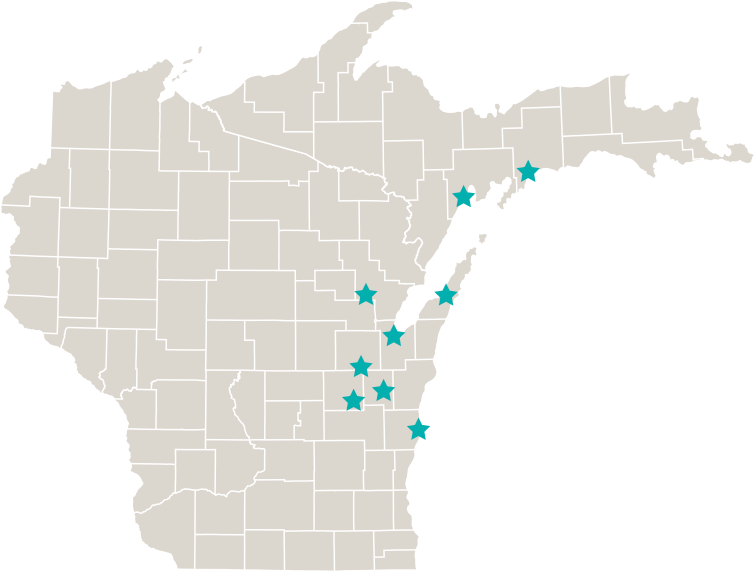
But not all of the benefits I just described are accessible to all the people of Wisconsin. Rural people, for instance, many of whom live fifty miles or more from cancer clinics, find the frequent travel a significant burden. It’s expensive and time consuming, at a time when they already don’t feel their best. Because cancer patients in rural Wisconsin have to spend more money traveling for care, they tend to forego screening and delay diagnosis. These delays cause rural cancer patients to be sicker, with more advanced disease when they finally do walk in the door—with worse survival rates as a result.
Sources: WI Office of Rural Health JCO Oncology Practice, Levit et Al, 7/6/2022 Health Services Research, Holmes et Al, 4/2006
Green Bay Oncology is well aware of this because we’ve driven to the moon and back—quite literally the distance from the earth to the moon, and back—taking cancer care closer to rural residents, so they can have a fair share of what they’ve already paid for with their tax dollars.
What Green Bay Oncology, in partnership with the American Cancer Society Cancer Action Network asks of our lawmakers is this:
- First, acknowledge the scope of the problem and the breadth of the people affected.
- Second, stay invested in the long game. From the frequent advertisements for new immunotherapy drugs you see on TV, you might get the impression that immunotherapy is a new idea, but I can tell you…immunotherapy for cancer was a hot topic all the way back when I was an undergraduate in the 1980s. All of today’s progress is a result of decades of basic science research – most of which was publicly funded. So mistrust anyone who promises quick results on the cheap.
- Third, don’t lose patience with the complexity of the problem. Yes, there are fantastic opportunities for private capital and public investment to work together, and yes—there\’s a role for research and regulatory reform. But there\’s no single, simple solution. We need public funds to support endeavors with little profit potential, and we need oversight and accountability anytime one group of people are tasked with spending other people\’s money. The key is balance, and balance is complex—not simple. Sensible, incremental change and progress gets the results. Slow and steady. That requires patience and persistence. Mistrust anyone shilling simple solutions.
- Fourth, let us help lawmakers identify and promote the most impactful reforms, and help craft a winning message to garner public support for the effort. The American Cancer Society Cancer Action Network and Green Bay Oncology understand that we only succeed together—lawmakers and healthcare leaders.
- Fifth, keep the door open for rural people, who cannot bridge the gap without expanded access to care
Only working together—clinicians, activists, and lawmakers—can we keep cancer treatment within reach of all the people of Wisconsin—rural, urban, or suburban. Much has been gained since the 1970s, and the people of Wisconsin have helped pay for that progress with their taxes. They rightly own a share of the returns.